1. Introduction and Background
Complex Post-Traumatic Stress Disorder (C-PTSD) is a distinct and challenging mental health condition that arises from prolonged exposure to traumatic events, often within the context of abusive relationships, captivity, or situations where individuals feel trapped and powerless
| [1] | Maercker, A., Brewin, C. R., Bryant, R. A., Cloitre, M., van Ommeren, M., Jones, L. M.,... & Reed, G. M. (2013). Proposals for mental disorders specifically associated with stress in the International Classification of Diseases-11. The Lancet, 381(9878), 1683-1685. https://doi.org/10.1016/S0140-6736(13)60578-3 |
[1]
. And it also called developmental PTSD
| [2] | Parthasarathy, A., Gupta, Alok. Partha's. (2021). Current Trends in Diagnosis & Management for Pediatric & Adolescent Practitioners.: Jaypee Brothers Medical Publishers Pvt. |
[2]
. In most cases, the traumatic experience is interpersonal which means that an individual might have experienced some chronic neglect, exposure to domestic violence or abuse at an early age. It’s also important to also note that chronic trauma can also take occur due to ongoing experiences such as bullying, undiagnosed or unsupported disability
| [3] | Attached Emily, Susan Anderson Emily (2021) Mental Health Workbook: 6 Books in 1: The Attachment Theory, Abandonment Anxiety, Depression in Relationships, Addiction, Complex PTSD, Trauma, CBT Therapy, EMDR and Somatic Psychotherapy. |
[3]
.
Unlike traditional Post-Traumatic Stress Disorder (PTSD), which typically results from isolated traumatic incidents, C-PTSD is rooted in chronic and cumulative trauma and encompasses a broader range of symptoms, including disturbances in self-identity, affect regulation, and interpersonal functioning
| [4] | Cloitre, M., Garvert, D. W., Weiss, B., Carlson, E. B., & Bryant, R. A. (2014). Distinguishing PTSD, complex PTSD, and borderline personality disorder: A latent class analysis. *European Journal of Psychotraumatology, 5*(1), 25097. https://doi.org/10.3402/ejpt.v5.25097 |
[4]
.
C-PTSD is characterized by a wide range of symptoms that encompass not only the core features of PTSD, such as intrusive memories, hyperarousal, and avoidance behaviors but also several additional symptoms that reflect disturbances in self-identity, affect regulation, and interpersonal functioning
| [4] | Cloitre, M., Garvert, D. W., Weiss, B., Carlson, E. B., & Bryant, R. A. (2014). Distinguishing PTSD, complex PTSD, and borderline personality disorder: A latent class analysis. *European Journal of Psychotraumatology, 5*(1), 25097. https://doi.org/10.3402/ejpt.v5.25097 |
[4]
. These additional symptoms include emotional dysregulation, profound feelings of shame and guilt, a distorted self-concept, and impaired relationships
| [4] | Cloitre, M., Garvert, D. W., Weiss, B., Carlson, E. B., & Bryant, R. A. (2014). Distinguishing PTSD, complex PTSD, and borderline personality disorder: A latent class analysis. *European Journal of Psychotraumatology, 5*(1), 25097. https://doi.org/10.3402/ejpt.v5.25097 |
| [5] | Karatzias, T., Hyland, P., Bradley, A., Cloitre, M., Roberts, N. P., Bisson, J. I., & Shevlin, M. (2017). Risk factors and comorbidity of ICD-11 PTSD and complex PTSD: Findings from a trauma-exposed population based sample of adults in the United Kingdom. Depression and Anxiety, 34(8), 814-824. https://doi.org/10.1002/da.22647 |
[4, 5]
. Survivors of complex trauma often exhibit dissociative symptoms as a coping mechanism to disconnect from overwhelming distress
| [6] | van der Kolk, B. A., Roth, S., Pelcovitz, D., Sunday, S., & Spinazzola, J. (2005). Disorders of extreme stress: The empirical foundation of a complex adaptation to trauma. *Journal of Traumatic Stress, 18*(5), 389-399. https://doi.org/10.1002/jts.20070 |
[6]
.
Impact of Complex Trauma on Psychological Well-being: Complex trauma, the primary cause of C-PTSD, typically involves prolonged exposure to multiple traumatic events, such as childhood abuse or domestic violence
| [7] | Courtois, C. A., & Ford, J. D. (2009). *Treating complex traumatic stress disorders: An evidence-based guide*. Guilford Press. |
[7]
. These traumatic experiences disrupt an individual's sense of safety and trust in others, leading to severe psychological and emotional consequences
| [7] | Courtois, C. A., & Ford, J. D. (2009). *Treating complex traumatic stress disorders: An evidence-based guide*. Guilford Press. |
[7]
. Research demonstrates that individuals with C-PTSD often experience more severe and enduring impairments in psychological well-being compared to those with traditional PTSD
| [8] | Herman, J. L. (1992). Complex PTSD: A syndrome in survivors of prolonged and repeated trauma. Journal of Traumatic Stress, 5(3), 377-391. |
[8]
. This impact includes severe mood disorders, such as depression and anxiety, along with a pervasive sense of hopelessness and worthlessness, which can lead to suicidal ideation and self-destructive behaviors
| [8] | Herman, J. L. (1992). Complex PTSD: A syndrome in survivors of prolonged and repeated trauma. Journal of Traumatic Stress, 5(3), 377-391. |
| [9] | Karatzias, T., Shevlin, M., Fyvie, C., Hyland, P., Efthymiadou, E., Wilson, D.,... & Cloitre, M. (2016). An initial psychometric assessment of an ICD-11 based measure of C-PTSD: The International Trauma Questionnaire. Journal of Anxiety, Stress, and Coping, 29(5), 561-574. https://doi.org/10.1080/10615806.2015.1100885 |
[8, 9]
.
People suffering from complex PTSD often suffer greatly from feelings of failure and worthlessness, which is why they often find it very difficult to act self- caring, feelings of guilt and shame occur
| [10] | Matten. Sven, Pausch, Markus (2024). Depression, Trauma, and Anxiety. Springer Nature. |
[10]
.
Distinguishing between C-PTSD and traditional PTSD is crucial for accurate diagnosis and effective treatment planning. While both conditions share some common features like flashbacks and hypervigilance, C-PTSD encompasses a broader range of symptoms that reflect the pervasive impact of chronic trauma on various aspects of a person's life
| [4] | Cloitre, M., Garvert, D. W., Weiss, B., Carlson, E. B., & Bryant, R. A. (2014). Distinguishing PTSD, complex PTSD, and borderline personality disorder: A latent class analysis. *European Journal of Psychotraumatology, 5*(1), 25097. https://doi.org/10.3402/ejpt.v5.25097 |
[4]
. One of the primary differences between PTSD and Complex PTSD is the duration and severity of the trauma. PTSD typically develops after a single traumatic event, while C- PTSD develops after prolonged or repeated exposure to trauma. Additionally, C- PTSD is often associated with developmental trauma, which can have a profound impact on a person's emotional and psychological development
| [11] | Thompson, M. (2024). Complex PTSD - The Time for Healing is Now. SAMUEL JORGE MARQUES CARTAXO. |
[11]
. One key distinguishing factor is the presence of disturbances in self-identity and interpersonal relationships, which are central to C-PTSD but less prominent in traditional PTSD
| [7] | Courtois, C. A., & Ford, J. D. (2009). *Treating complex traumatic stress disorders: An evidence-based guide*. Guilford Press. |
[7]
. Additionally, the course of recovery in C-PTSD often follows complex and protracted trajectories, necessitating specialized therapeutic approaches
| [12] | Cloitre, M., Courtois, C. A., Charuvastra, A., Carapezza, R., Stolbach, B. C., & Green, B. L. (2011). Treatment of complex PTSD: Results of the ISTSS expert clinician survey on best practices. *Journal of Traumatic Stress, 24*(6), 615-627. https://doi.org/10.1002/jts.20697 |
[12]
.
Diagnosing Complex PTSD (C-PTSD) is a crucial step in providing appropriate treatment and support to individuals who have experienced prolonged and cumulative trauma. The diagnosis of C-PTSD recognizes that the condition differs from traditional Post-Traumatic Stress Disorder (PTSD) due to its unique symptom profile, which includes not only the core features of PTSD, such as intrusive memories, hyperarousal, and avoidance behaviors but also additional symptoms related to disturbances in self-identity, affect regulation, and interpersonal functioning
| [4] | Cloitre, M., Garvert, D. W., Weiss, B., Carlson, E. B., & Bryant, R. A. (2014). Distinguishing PTSD, complex PTSD, and borderline personality disorder: A latent class analysis. *European Journal of Psychotraumatology, 5*(1), 25097. https://doi.org/10.3402/ejpt.v5.25097 |
[4]
.
To diagnose C-PTSD, mental health professionals typically follow diagnostic criteria, which may include:
1. Exposure to Prolonged Trauma: An individual must have a history of prolonged and cumulative traumatic experiences, such as chronic abuse, captivity, or interpersonal violence. These experiences often span an extended period, contributing to the complexity of the trauma
| [7] | Courtois, C. A., & Ford, J. D. (2009). *Treating complex traumatic stress disorders: An evidence-based guide*. Guilford Press. |
[7]
.
2. Core PTSD Symptoms: Individuals with C-PTSD will exhibit symptoms consistent with traditional PTSD, including intrusive memories, flashbacks, hypervigilance, and emotional reactivity
| [4] | Cloitre, M., Garvert, D. W., Weiss, B., Carlson, E. B., & Bryant, R. A. (2014). Distinguishing PTSD, complex PTSD, and borderline personality disorder: A latent class analysis. *European Journal of Psychotraumatology, 5*(1), 25097. https://doi.org/10.3402/ejpt.v5.25097 |
[4]
.
3. Additional Symptoms: The diagnosis of C-PTSD goes beyond the core PTSD symptoms to include the additional features associated with disturbances in self-identity, emotional regulation, and interpersonal relationships. These may manifest as feelings of worthlessness, shame, and difficulties in forming and maintaining relationships
| [4] | Cloitre, M., Garvert, D. W., Weiss, B., Carlson, E. B., & Bryant, R. A. (2014). Distinguishing PTSD, complex PTSD, and borderline personality disorder: A latent class analysis. *European Journal of Psychotraumatology, 5*(1), 25097. https://doi.org/10.3402/ejpt.v5.25097 |
[4]
.
4. Functional Impairment: To meet the diagnostic criteria, these symptoms must result in significant functional impairment in various areas of life, including work, social relationships, and overall well-being
| [5] | Karatzias, T., Hyland, P., Bradley, A., Cloitre, M., Roberts, N. P., Bisson, J. I., & Shevlin, M. (2017). Risk factors and comorbidity of ICD-11 PTSD and complex PTSD: Findings from a trauma-exposed population based sample of adults in the United Kingdom. Depression and Anxiety, 34(8), 814-824. https://doi.org/10.1002/da.22647 |
[5]
.
5. Duration: Symptoms must persist for an extended period, typically several months or more, reflecting the enduring nature of the condition
| [4] | Cloitre, M., Garvert, D. W., Weiss, B., Carlson, E. B., & Bryant, R. A. (2014). Distinguishing PTSD, complex PTSD, and borderline personality disorder: A latent class analysis. *European Journal of Psychotraumatology, 5*(1), 25097. https://doi.org/10.3402/ejpt.v5.25097 |
[4]
.
It is essential for mental health professionals to conduct a comprehensive clinical assessment to determine whether an individual meets the criteria for a C-PTSD diagnosis. Accurate diagnosis is fundamental to tailoring appropriate treatment approaches that address the multifaceted needs of individuals with C-PTSD.
Despite limited evidence, several therapies have shown promise in improving mental health outcomes and symptoms during this time frame. These therapies include Dialectical Behavioral Therapy (DBT) group skills training, Child Parent Psychotherapy, and multimodal therapeutic approaches at Mother-Baby Units (MBU)
| [13] | May, A., Balzan, R., Williams, A. S., Wade, T. D., & Paranjothy, S. M. (2023). Interventions for perinatal borderline personality disorder and complex trauma: A systematic review. *Archives of Women's Mental Health, 26*(3), 295–309. https://doi.org/10.1007/s00737-023-01313-4 |
[13]
.
Maercker and colleagues
| [14] | Maercker, A., Cloitre, M., Bachem, R., Schlumpf, Y. R., Khoury, B., Hitchcock, C., & Bohus, M. (2022). Complex post-traumatic stress disorder. *The Lancet, 400*(10345), 60–72. https://doi.org/10.1016/S0140-6736(22)00804-4 |
[14]
proposed treatment guidelines that suggest evidence-based approaches for complex PTSD. These approaches include trauma-focused interventions and multicomponent therapies. Multicomponent interventions that combine distress tolerance and emotional self-regulatory strategies with trauma-focused strategies have been shown to significantly reduce PTSD symptoms, emotional dysregulation, and interpersonal problems. It is crucial to develop individualized treatments based on specific needs and symptoms
| [14] | Maercker, A., Cloitre, M., Bachem, R., Schlumpf, Y. R., Khoury, B., Hitchcock, C., & Bohus, M. (2022). Complex post-traumatic stress disorder. *The Lancet, 400*(10345), 60–72. https://doi.org/10.1016/S0140-6736(22)00804-4 |
[14]
.
Trauma-focused cognitive behavioral therapy is recommended including children with complex PTSD considering comorbid symptoms, psychosocial functioning, coordination of services and social support
| [14] | Maercker, A., Cloitre, M., Bachem, R., Schlumpf, Y. R., Khoury, B., Hitchcock, C., & Bohus, M. (2022). Complex post-traumatic stress disorder. *The Lancet, 400*(10345), 60–72. https://doi.org/10.1016/S0140-6736(22)00804-4 |
[14]
.
A study by Simon et al.,
| [15] | Simon, N., Roberts, N. P., Lewis, C. E., van Gelderen, M. J., & Bisson, J. I. (2019). Associations between perceived social support, posttraumatic stress disorder (PTSD) and complex PTSD (C-PTSD): Implications for treatment. *European Journal of Psychotraumatology, 10*(1), 1573129. https://doi.org/10.1080/20008198.2019.1573129 |
[15]
asserted that those suffering from Complex PTSD experienced lower perceived social support than those without it. Therefore, intervention treatment methods should aim to improve their perceived support levels as it can significantly impact their relational functions, especially individuals who display disturbances
| [15] | Simon, N., Roberts, N. P., Lewis, C. E., van Gelderen, M. J., & Bisson, J. I. (2019). Associations between perceived social support, posttraumatic stress disorder (PTSD) and complex PTSD (C-PTSD): Implications for treatment. *European Journal of Psychotraumatology, 10*(1), 1573129. https://doi.org/10.1080/20008198.2019.1573129 |
[15]
.
Research indicates that currently, no gold standard exists concerning C-PTSD treatment procedures; however, keeping traumatic therapies such as cognitive-behavioral therapy (CBT), dialectical behavior therapy (DBT), or Prolonged Exposure (PE) must be retained while developing tailored approaches catering to individual needs
.
Ford and Courtois
| [17] | Ford, J. D., & Courtois, C. A. (2021). Complex PTSD and borderline personality disorder. *Borderline Personality Disorder and Emotion Dysregulation, 8*(1), 16. https://doi.org/10.1186/s40479-021-00155 |
[17]
respectfully delve into the nuances of treating complex posttraumatic stress disorder (C-PTSD) and borderline personality disorder (BPD) with psychotherapy. A suggestion is made that therapies like Mentalization Based Therapy (MBT) and Dialectical Behavior Therapy (DBT). Which directly addresses PTSD and C-PTSD symptoms. Can be enhanced when introducing therapeutic modalities for BPD and severe dissociation
| [17] | Ford, J. D., & Courtois, C. A. (2021). Complex PTSD and borderline personality disorder. *Borderline Personality Disorder and Emotion Dysregulation, 8*(1), 16. https://doi.org/10.1186/s40479-021-00155 |
[17]
.
Ter Heide, Mooren and Kleber
| [18] | Ter Heide, F. J., Mooren, T. M., & Kleber, R. J. (2016). Complex PTSD and phased treatment in refugees: A debate piece. *European Journal of Psychotraumatology, 7*, 28687. https://doi.org/10.3402/ejpt.v7.28687 |
[18]
recommend a phased treatment approach for refugees with PTSD by following sequential steps of safety assurance symptom reduction, skills training, processing traumatic memories or events along with social and psychological reintegration. The authors caution against stand-alone trauma-focused treatments without considering the specific needs of this population. They suggest culturally adapted cognitive behavioral therapy or narrative exposure therapy designed precisely to address the unique challenges faced by refugees.
| [18] | Ter Heide, F. J., Mooren, T. M., & Kleber, R. J. (2016). Complex PTSD and phased treatment in refugees: A debate piece. *European Journal of Psychotraumatology, 7*, 28687. https://doi.org/10.3402/ejpt.v7.28687 |
[18]
.
Interventions recommended during the reintegration phase of C-PTSD treatment include yoga exercises, service dog usage, residential treatment facilities that provide education options or self-defense classes along with patient research involvement opportunities. But these recommendations require further study to determine their effectiveness in treating this population effectively
| [19] | Purnell, L. R., Graham, A. C. J., Bloomfield, M. A. P., & Billings, J. (2021). Reintegration interventions for C-PTSD: A systematic review. *European Journal of Psychotraumatology, 12*(1), 1934789. https://doi.org/10.1080/20008198.2021.1934789 |
[19]
. As the understanding of C-PTSD evolves, innovative therapeutic approaches become essential to address its complexities.
One of the new approaches from the behavioral and cognitive wings that appears to be shifting the field in a different direction is Acceptance and Commitment Therapy (ACT)
ACT is a third-wave behavior therapy (Hayes et al, 1993). ACT is overtly contextualistic and is based on Relational Frame Theory (RFT), a fundamental experimental examination of human language and cognition. RFT explains why experience avoidance and cognitive fusion are pervasive and damaging. ACT focuses on these processes and is generating evidence that is favorable to both the processes and the results
. The core components of contextualism are a focus on the whole event, sensitivity to the role of context in understanding the nature and function of an event, and a firm grasp on a pragmatic truth criterion
| [21] | Snyder, C. R., & Ingram, R. E. (Eds.). (2000). *Handbook of psychological change: Psychotherapy processes & practices for the 21st century*. John Wiley & Sons, Inc. |
[21]
.
Acceptance and commitment therapy aims to increase psychological flexibility through the six basic principles as follows:
Acceptance: Embracing unwanted experiences: It means opening up to these experiences and allowing them to be as they are, in order to take steps towards chosen values. As such, the emphasis of acceptance is much more on behavioral qualities than emotional qualities
| [22] | Bennett, R., & Oliver, J. (2019). *Acceptance and commitment therapy: 100 key points and techniques.* Routledge. |
[22]
. Acceptance of private events is taught as an alternative to experiential avoidance. It involves the active and aware embrace of private events that are occasioned by our history, without unnecessary attempts to change their frequency or form, especially when doing so would cause psychological harm
| [23] | Luoma, J. B., Hayes, S. C., & Walser, R. D. (2007). *Learning ACT: An acceptance & commitment therapy skills-training manual for therapists*. New Harbinger Publications. |
[23]
.
Cognitive Defusion: Separating from negative thoughts: It refers to the human tendency to become entangled with thoughts as a result of a strong belief in their literal content. In other words, we listen to and believe what our minds tell us. It is the process by which we change our relationship with our thoughts by stepping back and simply witnessing their presence. When we defuse, we disentangle from our self-talk and observe cognitions as entities separate from ourselves—as just words. This allows us to look at our though
| [24] | Stoddard, J. A., & Afari, N. (2014). *The Big Book of ACT Metaphors: A practitioner's guide to experiential exercises and metaphors in Acceptance and Commitment Therapy*. New Harbinger Publications. |
[24]
. Fusion was related to PTSD through emotional non-clarity and fusion was related to goal dysregulation through emotional non-acceptance and PTSD
| [25] | Cox, D. W., Motl, T. C., Bakker, A. M., & Lunt, R. A. (2018). Cognitive fusion and post-trauma functioning in veterans: Examining the mediating roles of emotion dysregulation. *Journal of Contextual Behavioral Science, 8*, 1-7. https://doi.org/10.1016/j.jcbs.2017.11.001 |
[25]
.
Present-Moment Awareness: Mindfulness and Engagement: It defined as “paying attention in a particular way: on purpose, in the present moment, nonjudgmentally”
| [26] | Kabat-Zinn, J. (1994). Wherever you go, there you are: Mindfulness meditation in everyday life. Hyperion. |
[26]
Mindfulness-based treatments for posttraumatic stress disorder (PTSD) have emerged as promising adjunctive or alternative intervention approaches, mindfulness interventions may target emotional under- and overmodulation, both of which are critical features of PTSD symptomatology
| [27] | Boyd, J. E., Lanius, R. A., & McKinnon, M. C. (2018). Mindfulness-based treatments for posttraumatic stress disorder: A review of the treatment literature and neurobiological evidence. *Journal of Psychiatry & Neuroscience, 43*(1), 7–25. https://doi.org/10.1503/jpn.170021. |
[27]
.
Self-as-Context: Observing Inner Experiences: Gaining insight into a client’s ability to take perspective by observing the self as separate from their experiences and as a context for living experiences, rather than maintaining a rigid story of who one is throughout all contexts
| [28] | Twohig, M. P., Levin, M. E., & Petersen, J. M. (Eds.). (2023). *The Oxford handbook of acceptance and commitment therapy*. Oxford University Press. |
[28]
.
Identifying Values: Guiding Behavior with Purpose. Values are your heart’s deepest desires for how you want to behave as a human being. Values are not about what you want to get or achieve; they are about how you want to behave or act on an ongoing basis
| [29] | Harris, R. (2012). The reality slap: Finding peace and fulfillment when life hurts. New Harbinger Publications. |
[29]
.
Committed Action: Aligning Actions with Values. A committed action can be anything large or small that moves the client in the direction of his or her values, from simply getting up in the morning to the constellation of actions required to look for a new job. Committed action can also involve traditional behavior therapy strategies, such as exposure and response prevention
| [30] | Matthew S. Boone, Brian Mundy, Kate Morrissey Stahl & Bethany E. Genrich (2015): Acceptance and Commitment Therapy, Functional Contextualism, and Clinical Social Work, Journal of Human Behavior in the Social Environment, https://doi.org/10.1080/10911359.2015.1011255 |
[30]
.
Acceptance and Commitment Therapy (ACT) is gaining recognition for its versatility in addressing various mental health issues. In this comprehensive literature review, we delve into a collection of studies that underscore the potential of ACT as a valuable therapeutic approach.
Various studies have confirmed the effectiveness of ACT in the Context of Depression and anxiety: Kohtala et al.
| [31] | Kohtala, A., Lappalainen, R., Savonen, L., Timo, E., & Tolvanen, A. (2015). A four-session acceptance and commitment therapy based intervention for depressive symptoms delivered by masters degree level psychology students: A preliminary study. Behavioural and Cognitive Psychotherapy, 43(3), 360-373. https://doi.org/10.1017/S135246581400054X |
[31]
suggests that ACT can provide substantial relief for individuals experiencing depression, Zettle's work
extended this understanding by validating ACT's role in alleviating depression, primarily through enhancing psychological flexibility, Pots et al.
| [33] | Pots, W. T., Fledderus, M., Meulenbeek, P. A., ten Klooster, P. M., Schreurs, K. M., & Bohlmeijer, E. T. (2016). Acceptance and commitment therapy as a web-based intervention for depressive symptoms: Randomised controlled trial. *The British Journal of Psychiatry, 208*(1), 69-77. https://doi.org/10.1192/bjp.bp.114.151158 |
[33]
further expanded the horizons of ACT by exploring web-based public mental health interventions. in addition to Kyllönen et al.
| [34] | Kyllönen, H. M., Muotka, J., Puolakanaho, A., Astikainen, P., Keinonen, K., & Lappalainen, R. (2018). A brief acceptance and commitment therapy intervention for depression: A randomized controlled trial with 3-year follow-up for the intervention group. Journal of Contextual Behavioral Science, 10, 55-63. https://doi.org/10.1016/j.jcbs.2018.07.001 |
[34]
delved into the impact of a 6-hour ACT intervention delivered by novice therapists. Surprisingly, this study revealed significant improvements in clients struggling with depression. And Ferreira et al.
| [35] | Ferreira, M. G., Mariano, L. I., de Rezende, J. V., Caramelli, P., & Kishita, N. (2022). Effects of group Acceptance and Commitment Therapy (ACT) on anxiety and depressive symptoms in adults: A meta-analysis. *Journal of Affective Disorders, 309*, 297-308. https://doi.org/10.1016/j.jad.2022.04.077 |
[35]
contributed to the discourse by examining the efficacy of group-based ACT in addressing anxiety and depressive symptoms. Notably, their study hinted at ACT's advantage in mitigating depressive symptoms compared to other established treatments.
As for the efficacy ACT for Post-Traumatic Stress Disorder (PTSD): Orsillo and Batten
| [36] | Orsillo, S. M., & Batten, S. V. (2005). Acceptance and commitment therapy in the treatment of posttraumatic stress disorder. *Behavior Modification, 29*(1), 95-129. https://doi.org/10.1177/0145445504270876 |
[36]
initiated the application of ACT in the context of PTSD, featuring a compelling case example. This case illustrated how ACT effectively addressed life problems stemming from traumatic experiences, laying a solid foundation for understanding ACT's potential in mitigating the enduring impact of trauma. Michelle Woidneck, in collaboration with Utah State University, conducted a study assessing the utility of a 10-week ACT protocol for adolescents with PTSD
| [37] | Woidneck, M. R., Morrison, K. L., & Twohig, M. P. (2014). Acceptance and commitment therapy for the treatment of posttraumatic stress among adolescents. *Behavior Modification, 38*(4), 451–476. https://doi.org/10.1177/0145445513510527 |
[37]
. This investigation aimed to gauge both the effectiveness and acceptability of ACT in this population. Encouragingly, the results demonstrated a reduction in posttraumatic stress symptoms, along with improvements in measures of depression, general distress, and quality of life.
Fiorillo et al.
| [38] | Fiorillo, D., McLean, C., Pistorello, J., Hayes, S. C., & Follette, V. M. (2017). Evaluation of a web-based acceptance and commitment therapy program for women with trauma-related problems: A pilot study. *Journal of Contextual Behavioral Science, 6*(1), 104-113. https://doi.org/10.1016/j.jcbs.2017.01.001 |
[38]
extended the utility of ACT to participants grappling with PTSD, depression, and anxiety. This study showcased that ACT interventions not only increased participants' knowledge but also enhanced their psychological flexibility, yielding promising results for women survivors of interpersonal trauma. Phillips et al.
| [39] | Phillips, M. A., Chase, T., Bautista, C., Tang, A., & Teng, E. J. (2020). Using acceptance and commitment therapy techniques to enhance treatment engagement in veterans with posttraumatic stress disorder. *Bulletin of the Menninger Clinic, 84*(3), 264–277. https://doi.org/10.1521/bumc.2020.84.3.264 |
[39]
introduced adjunctive ACT techniques to enhance treatment engagement among veterans with PTSD, it discussed the potential of ACT techniques, such as cognitive defusion and values clarification, to promote participation in PTSD treatment, offering an innovative approach to improving engagement. Kelly et al.
| [40] | Kelly, M. M., Reilly, E. D., Ameral, V., Richter, S., & Fukuda, S. (2022). A randomized pilot study of acceptance and commitment therapy to improve social support for veterans with PTSD. Journal of Clinical Medicine, 11(12), 3482. https://doi.org/10.3390/jcm11123482 |
[40]
addressed the erosion of social support networks and interpersonal difficulties experienced by veterans with PTSD. Their pilot randomized trial assessed the efficacy of ACT in improving social support, resulting in significant enhancements in social relationships, engagement in social activities, and overall quality of life.
ACT for PTSD: A Paradigm Shift: Traditionally, PTSD has been conceptualized as an anxiety disorder primarily associated with fear and anxiety responses triggered by specific traumatic events. Effective treatments for PTSD, such as exposure therapy, have been rooted in this fear-based model. However, a paradigm shift is underway, with some researchers arguing that PTSD is fundamentally a disorder of experiential avoidance
| [41] | Batten, S. V., & Hayes, S. C. (2005). Acceptance and Commitment Therapy in the treatment of comorbid substance abuse and post-traumatic stress disorder: A case study. *Clinical Case Studies, 4*(3), 246–262. https://doi.org/10.1177/1534650103259689 |
[41]
. Within this evolving framework, acceptance-based behavioral therapies like ACT have gained prominence, aiming to enhance the effectiveness and comprehensiveness of PTSD treatment by addressing the avoidance behaviors and experiential avoidance at the core of the disorder
| [36] | Orsillo, S. M., & Batten, S. V. (2005). Acceptance and commitment therapy in the treatment of posttraumatic stress disorder. *Behavior Modification, 29*(1), 95-129. https://doi.org/10.1177/0145445504270876 |
[36]
.
ACT for Trauma and PTSD: An Empirical Review: Bean et al.
| [42] | Bean, R. C., Ong, C. W., Lee, J., & Twohig, M. P. (2017). Acceptance and commitment therapy for PTSD and trauma: An empirical review. *Behavior Therapy, 48*(3), 145-150. https://doi.org/10.1016/j.beth.2016.11.001 |
[42]
conducted an empirical review to summarize the existing data on the application of ACT to trauma and PTSD. Although the field is still in its early stages, preliminary evidence suggests that ACT holds promise as an effective intervention. However, the authors highlight the need for more extensive clinical trials that examine the effectiveness of ACT across diverse trauma presentations and client variables.
ACT Group Therapy for Non-Military Women with PTSD: Rachel DeLateur
conducted a study to investigate the effectiveness of ACT in a group setting over eight weeks for women diagnosed with PTSD due to childhood trauma. The findings were compelling, showing a significant decrease in PTSD symptoms measured using the PTSD checklist-civilian (PCL-C). This research contributes to social change by potentially reducing suicidal thoughts and behaviors, enhancing overall functioning, and promoting prosocial behaviors.
Group-Based ACT for Trauma Survivors: Spidel et al.
| [44] | Spidel, A., Daigneault, I., Kealy, D., & Lecomte, T. (2019). Acceptance and commitment therapy for psychosis and trauma: Investigating links between trauma severity, attachment, and outcome. *Behavioural and Cognitive Psychotherapy, 47*(2), 230-243. https://doi.org/10.1017/S1352465818000413 |
[44]
explored the effectiveness of group-based ACT for individuals with a history of trauma and psychosis, irrespective of trauma severity. Their findings suggested that the brevity of the intervention did not diminish its promise, emphasizing the importance of consistent attendance to maximize therapeutic benefits.
Comparing ACT and Trauma-Focused Cognitive Behavioral Therapy (TF CBT): Colleen M. Kirsch Hiltz White
| [45] | Kirsch Hiltz White, C. M. (2020). Comparison study: Trauma-focused cognitive behavioral therapy and acceptance and commitment therapy for trauma. |
[45]
addressed the need for evidence-based treatments for adolescents with trauma-related disorders. In a comparison study, they directly evaluated six weeks of Acceptance and Commitment Therapy for Trauma against Trauma-Focused Cognitive Behavioral Therapy (TF CBT) via telehealth during the COVID-19 pandemic. The results indicated that both treatments were effective in reducing trauma-related symptoms in adolescent participants.
ACT in Intensive Outpatient Programs: Ramirez et al.
| [46] | Ramirez, M. W., Woodworth, C. A., Evans, W. R., Grace, G. A., Schobitz, R. P., Villarreal, S. A., Howells, C. J., Gissendanner, R. D., Katko, N. J., Jones, K. N., McCabe, A. E., & Terrell, D. J. (2021). A trauma-focused intensive outpatient program integrating elements of exposure therapy with acceptance and commitment therapy: Program development and initial outcomes. *Journal of Contextual Behavioral Science, 21*, 66-72. https://doi.org/10.1016/j.jcbs.2021.06.002 |
[46]
described the development of an intensive outpatient program that integrated elements of exposure therapy with ACT for military-related PTSD. This innovative program yielded substantial reductions in PTSD symptoms, demonstrating the feasibility and effectiveness of combining ACT with established PTSD treatments.
ACT and Post-Traumatic Growth: While PTSD treatment primarily focuses on symptom reduction, Troxel-Galang
| [47] | Troxel-Galang, A. (2021). *The efficacy of a spiritual acceptance and commitment therapy protocol for post-traumatic growth* (Unpublished doctoral dissertation). The Wright Institute. |
[47]
delved into the potential of ACT, combined with spiritual practices, to promote post-traumatic growth. The study reported significant gains in post-traumatic growth, increased spiritual well-being, and a decrease in posttraumatic stress symptoms, underlining the importance of holistic approaches.
Integrating ACT within Trauma-Focused Therapies: The integration of ACT techniques within traditional trauma-focused therapies is an ongoing exploration. Glass
| [48] | Glass, R. (2022). The Blending of Cognitive Processing Therapy and Acceptance and Commitment Therapy to Address Trauma and PTSD. Widener University. |
[48]
proposed this integration within Cognitive Processing Therapy (CPT) to enhance trauma treatment. The approach aimed to manage distress associated with imagine exposure, providing insights into the potential synergies between ACT and traditional trauma-focused therapies.
One such groundbreaking approach is Trauma-Focused Acceptance and Commitment Therapy (TF-ACT), which integrates the principles of Acceptance and Commitment Therapy (ACT) with specialized techniques tailored to trauma survivors
| [49] | Harris, R. (2021). Trauma-Focused ACT: A Practitioner's Guide to Working with Mind, Body, and Emotion Using Acceptance and Commitment Therapy. Context Press, USA. |
[49]
. TF-ACT acknowledges the multifaceted nature of trauma and offers a holistic framework that aligns seamlessly with the unique characteristics and needs of individuals living with C-PTSD. This innovative therapy leverages insights from evolutionary science, Polyvagal Theory, Attachment Theory, and Inhibitory Learning Theory to provide a comprehensive and adaptable approach to trauma recovery
| [49] | Harris, R. (2021). Trauma-Focused ACT: A Practitioner's Guide to Working with Mind, Body, and Emotion Using Acceptance and Commitment Therapy. Context Press, USA. |
[49]
.
Trauma-Focused Acceptance and Commitment Therapy (TF-ACT): Integration and Specialization:
Trauma can leave deep emotional scars, affecting individuals on multiple levels. Trauma-Focused Acceptance and Commitment Therapy (TF-ACT) emerges as a specialized therapeutic approach that combines the foundational principles of Acceptance and Commitment Therapy (ACT) with targeted strategies to address trauma-related issues comprehensively. This integration of ACT principles with specialized trauma techniques makes TF-ACT a powerful tool in the therapeutic landscape
| [49] | Harris, R. (2021). Trauma-Focused ACT: A Practitioner's Guide to Working with Mind, Body, and Emotion Using Acceptance and Commitment Therapy. Context Press, USA. |
[49]
.
TF-ACT: An Extension of ACT for Trauma-Related Issues:
Acceptance and Commitment Therapy (ACT) provides the philosophical underpinning for TF-ACT. ACT's core components include psychological flexibility, mindfulness, values clarification, and committed action. These elements, rooted in the acceptance of internal experiences and alignment with personal values, serve as the foundation for TF-ACT's approach to healing trauma.
| [49] | Harris, R. (2021). Trauma-Focused ACT: A Practitioner's Guide to Working with Mind, Body, and Emotion Using Acceptance and Commitment Therapy. Context Press, USA. |
[49]
.
TF-ACT recognizes the need for a specialized approach to address trauma-related issues. Trauma can lead to a range of psychological and physiological responses, including hyperarousal, intrusive memories, and emotional dysregulation. To effectively address these issues, TF-ACT integrates insights from various disciplines, including evolutionary science, Polyvagal Theory, Attachment Theory, and Inhibitory Learning Theory
| [49] | Harris, R. (2021). Trauma-Focused ACT: A Practitioner's Guide to Working with Mind, Body, and Emotion Using Acceptance and Commitment Therapy. Context Press, USA. |
[49]
.
Incorporation of Evolutionary Science, Polyvagal Theory, Attachment Theory, Inhibitory Learning Theory:
Evolutionary science provides insights into the survival mechanisms that underlie trauma responses. TF-ACT acknowledges the role of these survival mechanisms and helps individuals understand how their reactions to trauma are rooted in the evolutionary imperative to protect oneself from harm.
| [49] | Harris, R. (2021). Trauma-Focused ACT: A Practitioner's Guide to Working with Mind, Body, and Emotion Using Acceptance and Commitment Therapy. Context Press, USA. |
[49]
.
Polyvagal Theory, developed by Stephen Porges, informs TF-ACT's approach to understanding the nervous system's responses to trauma. By recognizing the interplay between the sympathetic and parasympathetic branches of the autonomic nervous system, TF-ACT helps clients regulate their physiological responses and regain a sense of safety
| [49] | Harris, R. (2021). Trauma-Focused ACT: A Practitioner's Guide to Working with Mind, Body, and Emotion Using Acceptance and Commitment Therapy. Context Press, USA. |
[49]
.
Attachment Theory is another crucial component of TF-ACT. It acknowledges the profound impact of attachment experiences on an individual's response to trauma. Clients are guided to explore their attachment styles and how these styles may influence their relationships and reactions to trauma-related triggers
| [49] | Harris, R. (2021). Trauma-Focused ACT: A Practitioner's Guide to Working with Mind, Body, and Emotion Using Acceptance and Commitment Therapy. Context Press, USA. |
[49]
.
Inhibitory Learning Theory, drawn from the field of behavioral psychology, informs TF-ACT's strategies for addressing traumatic memories and associations. By targeting the mechanisms through which fear is acquired and maintained, TF-ACT helps clients reevaluate and recontextualize traumatic memories, reducing their emotional charge
| [49] | Harris, R. (2021). Trauma-Focused ACT: A Practitioner's Guide to Working with Mind, Body, and Emotion Using Acceptance and Commitment Therapy. Context Press, USA. |
[49]
.
Therapeutic Components of Trauma-Focused ACT:
Emphasizing the Present Moment: Living, Healing, and Building:
TF-ACT's therapeutic journey unfolds across three fundamental phases: living in the present, healing the past, and building the future. Each phase comprises specific strategies and techniques aimed at addressing trauma-related challenges
| [49] | Harris, R. (2021). Trauma-Focused ACT: A Practitioner's Guide to Working with Mind, Body, and Emotion Using Acceptance and Commitment Therapy. Context Press, USA. |
[49]
.
Living in the Present: Overcoming Hyperarousal and Embracing Self-Compassion:
The initial phase, "Living in the Present," is a crucial starting point in trauma recovery. Trauma often leaves individuals in a state of hyperarousal, characterized by heightened vigilance and emotional reactivity. TF-ACT introduces mindfulness practices to help clients ground themselves in the present moment. This mindfulness enables individuals to observe their thoughts and sensations without judgment, reducing the grip of traumatic memories
| [49] | Harris, R. (2021). Trauma-Focused ACT: A Practitioner's Guide to Working with Mind, Body, and Emotion Using Acceptance and Commitment Therapy. Context Press, USA. |
[49]
.
Self-compassion is another cornerstone of this phase. TF-ACT encourages clients to treat themselves with kindness and understanding, counteracting the self-blame often associated with trauma. By fostering self-compassion, individuals can begin to alleviate the emotional burdens carried from the past
| [49] | Harris, R. (2021). Trauma-Focused ACT: A Practitioner's Guide to Working with Mind, Body, and Emotion Using Acceptance and Commitment Therapy. Context Press, USA. |
[49]
.
Healing the Past: Techniques for Addressing Past-Oriented Cognitions:
The second phase, "Healing the Past," delves into addressing past-oriented cognitions. Trauma often leads to intrusive memories, flashbacks, and negative beliefs about oneself and the world. TF-ACT employs strategies such as defusion to help clients distance themselves from distressing thoughts and memories. This defusion enables clients to recognize that these thoughts are not absolute truths, reducing their emotional impact
| [49] | Harris, R. (2021). Trauma-Focused ACT: A Practitioner's Guide to Working with Mind, Body, and Emotion Using Acceptance and Commitment Therapy. Context Press, USA. |
[49]
.
TF-ACT also leverages acceptance, helping clients acknowledge their traumatic experiences without judgment. Clients learn to make room for their pain and distress, creating a safe space for emotional processing. This phase may also involve somatic techniques to address the physical manifestations of trauma
| [49] | Harris, R. (2021). Trauma-Focused ACT: A Practitioner's Guide to Working with Mind, Body, and Emotion Using Acceptance and Commitment Therapy. Context Press, USA. |
[49]
.
Building the Future: Values-Based Goal Setting and Planning:
The final phase, "Building the Future," focuses on setting goals and taking committed actions aligned with one's values. TF-ACT guides clients in clarifying their core values, the principles that guide their lives. These values become the compass for making choices and setting meaningful goals
| [49] | Harris, R. (2021). Trauma-Focused ACT: A Practitioner's Guide to Working with Mind, Body, and Emotion Using Acceptance and Commitment Therapy. Context Press, USA. |
[49]
.
Clients are empowered to take concrete steps toward their chosen values, even in the face of discomfort or triggers. TF-ACT emphasizes that trauma should not dictate one's future but instead serves as a motivation to build a life in alignment with personal values
| [49] | Harris, R. (2021). Trauma-Focused ACT: A Practitioner's Guide to Working with Mind, Body, and Emotion Using Acceptance and Commitment Therapy. Context Press, USA. |
[49]
.
The Multidimensional Approach of TF-ACT: Integrating Somatic and Cognitive Strategies:
TF-ACT recognizes that trauma is not solely a cognitive experience; it deeply affects the body as well. As a result, TF-ACT integrates somatic strategies to address the physical aspects of trauma. Clients are guided to become aware of bodily sensations and learn grounding techniques to enhance their connection to the present moment
| [49] | Harris, R. (2021). Trauma-Focused ACT: A Practitioner's Guide to Working with Mind, Body, and Emotion Using Acceptance and Commitment Therapy. Context Press, USA. |
[49]
.
Adaptability and Flexibility in TF-ACT: Tailoring to Individual Needs:
Perhaps one of TF-ACT's most significant strengths lies in its adaptability and flexibility. The therapy is not a rigid, one-size-fits-all approach but a dynamic framework that can be tailored to meet individual needs. This adaptability extends to the pace of therapy, allowing clients to progress at their own speed, whether they require short-term or extended support
| [49] | Harris, R. (2021). Trauma-Focused ACT: A Practitioner's Guide to Working with Mind, Body, and Emotion Using Acceptance and Commitment Therapy. Context Press, USA. |
[49]
.
TF-ACT therapists are skilled in customizing therapy sessions based on clients' specific challenges and preferences. Some clients may benefit from structured activities, while others may find value in open-ended discussions. This personalized approach ensures that clients receive the most effective and relevant support throughout their healing journey
| [49] | Harris, R. (2021). Trauma-Focused ACT: A Practitioner's Guide to Working with Mind, Body, and Emotion Using Acceptance and Commitment Therapy. Context Press, USA. |
[49]
.
In conclusion, Trauma-Focused Acceptance and Commitment Therapy (TF-ACT) represents a sophisticated integration of ACT principles with specialized trauma techniques. Drawing from insights in evolutionary science, Polyvagal Theory, Attachment Theory, and Inhibitory Learning Theory, TF-ACT offers a holistic approach to trauma recovery. Its emphasis on living in the present, healing the past, and building the future, along with the integration of somatic strategies, makes TF-ACT a comprehensive and adaptable therapeutic approach that can be tailored to each individual's unique needs. Ultimately, TF-ACT empowers individuals to heal from trauma, regain control over their lives, and build a future in alignment with their values and well-being.
Relevance of Trauma-Focused Acceptance and Commitment Therapy (TF-ACT) in Complex PTSD Treatment:
Complex Post-Traumatic Stress Disorder (Complex PTSD or C-PTSD) is a distinct condition that arises from prolonged exposure to traumatic events, often occurring within the context of abusive relationships, captivity, or situations where individuals feel trapped and powerless
| [1] | Maercker, A., Brewin, C. R., Bryant, R. A., Cloitre, M., van Ommeren, M., Jones, L. M.,... & Reed, G. M. (2013). Proposals for mental disorders specifically associated with stress in the International Classification of Diseases-11. The Lancet, 381(9878), 1683-1685. https://doi.org/10.1016/S0140-6736(13)60578-3 |
[1]
. It differs from traditional PTSD in that it encompasses a broader range of symptoms, including disturbances in self-identity, affect regulation, and interpersonal functioning
| [4] | Cloitre, M., Garvert, D. W., Weiss, B., Carlson, E. B., & Bryant, R. A. (2014). Distinguishing PTSD, complex PTSD, and borderline personality disorder: A latent class analysis. *European Journal of Psychotraumatology, 5*(1), 25097. https://doi.org/10.3402/ejpt.v5.25097 |
[4]
. The distinctive features of Complex PTSD necessitate specialized therapeutic approaches, making Trauma-Focused Acceptance and Commitment Therapy (TF-ACT) particularly relevant due to its alignment with these characteristics
| [49] | Harris, R. (2021). Trauma-Focused ACT: A Practitioner's Guide to Working with Mind, Body, and Emotion Using Acceptance and Commitment Therapy. Context Press, USA. |
[49]
.
TF-ACT's Alignment with Complex PTSD Characteristics:
Complex PTSD is marked by disruptions in self-identity, emotional dysregulation, and pervasive feelings of shame and guilt
| [4] | Cloitre, M., Garvert, D. W., Weiss, B., Carlson, E. B., & Bryant, R. A. (2014). Distinguishing PTSD, complex PTSD, and borderline personality disorder: A latent class analysis. *European Journal of Psychotraumatology, 5*(1), 25097. https://doi.org/10.3402/ejpt.v5.25097 |
[4]
. TF-ACT's foundations in mindfulness and self-compassion align seamlessly with the needs of individuals grappling with these identity-related challenges
. Through mindfulness practices integrated into the "Living in the Present" phase, TF-ACT assists clients in grounding themselves in the here and now, reducing emotional reactivity, and cultivating emotional regulation skills.
| [49] | Harris, R. (2021). Trauma-Focused ACT: A Practitioner's Guide to Working with Mind, Body, and Emotion Using Acceptance and Commitment Therapy. Context Press, USA. |
[49]
. Simultaneously, by promoting self-compassion, it addresses the self-blame and self-criticism often intertwined with Complex PTSD
| [49] | Harris, R. (2021). Trauma-Focused ACT: A Practitioner's Guide to Working with Mind, Body, and Emotion Using Acceptance and Commitment Therapy. Context Press, USA. |
[49]
.
Furthermore, TF-ACT draws from Polyvagal Theory to help individuals regulate their physiological responses, which is pivotal in addressing emotional dysregulation, a common feature of Complex PTSD. By providing tools to manage hyperarousal and intrusive memories, TF-ACT effectively targets the core symptoms of Complex PTSD.
Leveraging TF-ACT's Approach for Comprehensive Healing:
TF-ACT's comprehensive three-phase approach—living in the present, healing the past, and building the future—provides a robust framework to address the multifaceted nature of Complex PTSD
| [8] | Herman, J. L. (1992). Complex PTSD: A syndrome in survivors of prolonged and repeated trauma. Journal of Traumatic Stress, 5(3), 377-391. |
[8]
. In the "Living in the Present" phase, the emphasis on mindfulness and self-compassion aids individuals in reestablishing a sense of self amid the aftermath of trauma
| [49] | Harris, R. (2021). Trauma-Focused ACT: A Practitioner's Guide to Working with Mind, Body, and Emotion Using Acceptance and Commitment Therapy. Context Press, USA. |
[49]
.
By encouraging clients to accept their emotional experiences without judgment, TF-ACT addresses the profound shame and guilt often intertwined with Complex PTSD.
Transitioning to the "Healing the Past" phase, TF-ACT directly confronts traumatic memories and negative self-beliefs, which are pervasive in Complex PTSD. Techniques like defusion and acceptance empower clients to detach from distressing thoughts, thereby alleviating their emotional impact. Somatic techniques can be incorporated to address the physical tension associated with trauma
| [49] | Harris, R. (2021). Trauma-Focused ACT: A Practitioner's Guide to Working with Mind, Body, and Emotion Using Acceptance and Commitment Therapy. Context Press, USA. |
[49]
.
The "Building the Future" phase focuses on values-based goal setting and committed action, aligning with the potential for post-traumatic growth in individuals with Complex PTSD. It empowers clients to envision a future that is not solely defined by their trauma but is instead shaped by their values and aspirations
| [49] | Harris, R. (2021). Trauma-Focused ACT: A Practitioner's Guide to Working with Mind, Body, and Emotion Using Acceptance and Commitment Therapy. Context Press, USA. |
[49]
.
Promising Outcomes and Potential for Post-Traumatic Growth:
Research has demonstrated promising outcomes for individuals with Complex PTSD who engage in trauma-focused therapies
| [5] | Karatzias, T., Hyland, P., Bradley, A., Cloitre, M., Roberts, N. P., Bisson, J. I., & Shevlin, M. (2017). Risk factors and comorbidity of ICD-11 PTSD and complex PTSD: Findings from a trauma-exposed population based sample of adults in the United Kingdom. Depression and Anxiety, 34(8), 814-824. https://doi.org/10.1002/da.22647 |
[5]
. TF-ACT's adaptability and flexibility make it particularly suitable to accommodate the varying needs and trajectories of individuals with Complex PTSD
| [49] | Harris, R. (2021). Trauma-Focused ACT: A Practitioner's Guide to Working with Mind, Body, and Emotion Using Acceptance and Commitment Therapy. Context Press, USA. |
| [50] | Neff, K. D. (2003). Development and validation of a scale to measure self-compassion. *Self and Identity, 2*(3), 223-250. https://doi.org/10.1080/15298860309027 |
| [51] | Cloitre, M., Courtois, C. A., Ford, J. D., Green, B. L., Alexander, P., Briere, J.,... & van der Hart, O. (2011). The ISTSS Expert Consensus Treatment Guidelines for Complex PTSD in adults. Retrieved from https://www.istss.org/ISTSS_Main/media/Documents/ISTSS-Expert-Concesnsus-Guidelines-for-Complex-PTSD-Updated-060315.pdf |
[49-51]
. Beyond mere symptom reduction, TF-ACT recognizes the potential for post-traumatic growth, enabling individuals to find meaning and growth even in the aftermath of profound adversity
. By guiding clients to align their actions with their core values in the "Building the Future" phase, TF-ACT fosters resilience and the capacity for post-traumatic growth
| [49] | Harris, R. (2021). Trauma-Focused ACT: A Practitioner's Guide to Working with Mind, Body, and Emotion Using Acceptance and Commitment Therapy. Context Press, USA. |
[49]
.
In conclusion, Trauma-Focused Acceptance and Commitment Therapy (TF-ACT) is highly relevant in the treatment of Complex PTSD (C-PTSD) due to its alignment with the condition's characteristics, comprehensive approach to healing, and potential for post-traumatic growth. This therapeutic approach effectively addresses the emotional dysregulation, disturbances in self-identity, and challenges in relationships often experienced by individuals with Complex PTSD, offering a promising path to recovery, resilience, and personal growth.
1.1. Research Questions
This study aims to investigate the effectiveness and versatility of Trauma-Focused Acceptance and Commitment Therapy (TF-ACT) in addressing the complex and multifaceted nature of Complex Post-Traumatic Stress Disorder (C-PTSD).
Specific research questions:
1. How does TF-ACT effectively alleviate the unique symptoms and challenges associated with Complex Post-Traumatic Stress Disorder (C-PTSD)?
2. To what extent can TF-ACT promote post-traumatic growth and recovery in individuals who have experienced prolonged trauma and adversity?
3. What role can TF-ACT play in enhancing self-identity, affect regulation, and interpersonal functioning in individuals with C-PTSD?
4. How does TF-ACT compare to other therapeutic approaches in the treatment of C-PTSD?
1.2. Hypotheses to Be Tested
We hypothesize the following:
1. TF-ACT will significantly reduce the symptoms associated with Complex Post-Traumatic Stress Disorder (C-PTSD), including disturbances in self-identity, affect regulation, and interpersonal functioning.
2. TF-ACT will foster post-traumatic growth and recovery in individuals with C-PTSD by providing them with valuable tools to reclaim their lives and well-being.
3. TF-ACT will effectively address the unique challenges posed by C-PTSD, such as pervasive feelings of shame, guilt, and mistrust.
4. TF-ACT will demonstrate comparable or superior outcomes compared to other therapeutic approaches commonly used in the treatment of C-PTSD.
1.3. Significance of the Study
This study holds profound significance in the field of mental health, particularly in the context of Complex Post-Traumatic Stress Disorder (C-PTSD). By focusing on Trauma-Focused Acceptance and Commitment Therapy (TF-ACT) and its application in addressing the complexities of C-PTSD, this research aims to:
1. Provide a deeper understanding of how TF-ACT can effectively alleviate the symptoms and challenges associated with C-PTSD.
2. Contribute empirical evidence on the role of TF-ACT in promoting post-traumatic growth and recovery.
3. Enhance the therapeutic options available for individuals living with C-PTSD.
4. Explore the potential of TF-ACT to improve self-identity, affect regulation, and interpersonal functioning in the context of C-PTSD.
2. Methodology
2.1. Objective
The primary objective of this study is to investigate the effectiveness of Trauma-Focused Acceptance and Commitment Therapy (TF-ACT) in reducing symptoms of Complex PTSD in a specific patient. Additionally, the study aimed to delve into the therapeutic process, outcomes, and enhancements observed during the intervention through a mixed methods approach.
2.2. Research Design
This study employed a single case study mixed methods to assessed the efficacy of Trauma-Focused Acceptance and Commitment Therapy (TF-ACT) in alleviating symptoms associated with Complex PTSD. The research design integrated quantitative and qualitative data collection and analysis, offering a comprehensive understanding of the therapeutic process and outcomes. Specifically, this research utilized a Single case study–mixed methods (SCS-MM) approach, wherein a primary case study is embedded within a nested mixed methods framework.
The data triangulation strategy was used to give greater credibility to the results (Cresswell, 2011), where different types of data were collected from different sources from different tools (a questionnaire, interview, and case study).
2.3. Participant
The participant in this study is a 39-year-old married female patient diagnosed with Complex PTSD. The participant's traumatic experiences encompass a turbulent childhood characterized by abuse, abandonment, and violence, along with exposure to war-related trauma in adulthood. Despite her outward appearance as a dedicated wife, mother of four, and university graduate, her life has been marked by a relentless struggle with C-PTSD. Her journey reveals the profound and intricate challenges of this condition.
Tumultuous Early Years: The client's ordeal began in childhood, characterized by an authoritarian father whose emotional rigidity stemmed from his own violent upbringing. Despite the family's considerable wealth, she found no refuge from emotional turmoil. A particularly traumatic memory from age 8 involves being abandoned with her sister on a stormy night after their car broke down. The memory of their tears mingling with the rain remains vivid. Subsequent years were marked by brutal physical abuse. At ages 9 and 10, she endured harrowing episodes of violence from her father, leading to sleepless nights. By age 12, the cruelty reached its peak when her father whipped her while she was tied to a pole.
The Adolescent Struggle: The cycle of violence continued through adolescence, with ages 13 to 15 marked by successive brutalities, deepening both physical and emotional scars. At 16, she witnessed her mother being severely beaten, adding another layer of anguish.
Entering Adulthood: Adulthood offered little respite. At 19, she married, only to face the horrors of the 2008 war. Bombings and shelling became her stark reality, and neighboring homes' collapses showered her with shattered glass as she sought refuge. Subsequent wars in 2012 and 2014 amplified her trauma. The psychological anguish worsened with the loss of her cherished aunt, a confidante with whom she shared a profound bond.
The Breaking Point: By 2020, the ceaseless psychological torment became unbearable. Her past scars and present horrors intertwined, creating an intricate tapestry of pain. The wars of 2021 and 2022 triggered a surge in PTSD symptoms, profoundly disrupting her psychological, social, and familial spheres.
Symptomatology: The client exhibits a multitude of symptoms characteristic of C-PTSD:
1) Avoidance: She avoids reminders of her traumatic past, evading situations that recall painful memories.
2) Physical Reactions: Recollections of trauma induce dizziness and nausea.
3) Hyperarousal: She remains in a perpetual state of high alert.
4) Trust Erosion: Trust in herself and others has diminished.
5) Sleep and Concentration Challenges: She experiences sleeplessness and concentration difficulties.
Additionally, C-PTSD introduces the following challenges:
1) Negative Self-View: She grapples with feelings of helplessness, guilt, and shame.
2) Worldview Transformation: Her perspective on the world has darkened.
3) Emotional Turmoil: She struggles to control intense emotions, including anger and sadness.
4) Strained Relationships: Her capacity to trust and engage in healthy relationships has waned.
5) Detachment and Preoccupation: She experiences either detachment from painful memories or fixation on the abuser.
Diagnosis and the Path to Healing: This case exemplifies the enduring impact of prolonged and recurrent trauma, etched across her life from childhood into adulthood. Her diagnosis of C-PTSD highlights the challenges in addressing trauma that extends beyond traditional PTSD boundaries.
The journey toward healing and recovery, guided by compassionate healthcare professionals, promises a brighter, more resilient future. This case demonstrates the potential for recovery even in the face of profound trauma, illuminating a path from darkness to hope.
2.4. Tools
2.4.1. Quantitative Tools
The International Trauma Questionnaire (ITQ) for PTSD: The International Trauma Questionnaire (ITQ) is a valuable tool used in the assessment and diagnosis of both traditional PTSD and Complex PTSD
| [9] | Karatzias, T., Shevlin, M., Fyvie, C., Hyland, P., Efthymiadou, E., Wilson, D.,... & Cloitre, M. (2016). An initial psychometric assessment of an ICD-11 based measure of C-PTSD: The International Trauma Questionnaire. Journal of Anxiety, Stress, and Coping, 29(5), 561-574. https://doi.org/10.1080/10615806.2015.1100885 |
[9]
Developed by experts in the field, the ITQ provides a standardized and structured approach to evaluate the presence and severity of trauma-related symptoms in accordance with the diagnostic criteria outlined in the International Classification of Diseases, 11th Revision (ICD-11)
| [9] | Karatzias, T., Shevlin, M., Fyvie, C., Hyland, P., Efthymiadou, E., Wilson, D.,... & Cloitre, M. (2016). An initial psychometric assessment of an ICD-11 based measure of C-PTSD: The International Trauma Questionnaire. Journal of Anxiety, Stress, and Coping, 29(5), 561-574. https://doi.org/10.1080/10615806.2015.1100885 |
[9]
. The ITQ consists of a series of questions and prompts designed to elicit information about an individual's traumatic experiences and their emotional and psychological responses to those experiences. It assesses not only the core symptoms of PTSD but also the additional symptoms associated with disturbances in self-identity and interpersonal functioning that are characteristic of Complex PTSD
| [4] | Cloitre, M., Garvert, D. W., Weiss, B., Carlson, E. B., & Bryant, R. A. (2014). Distinguishing PTSD, complex PTSD, and borderline personality disorder: A latent class analysis. *European Journal of Psychotraumatology, 5*(1), 25097. https://doi.org/10.3402/ejpt.v5.25097 |
[4]
. The questionnaire can be administered by trained mental health professionals and assists in the systematic evaluation of trauma-related symptoms, helping to determine whether an individual meets the criteria for a C-PTSD diagnosis as outlined in the ICD-11. The use of standardized assessment tools like the ITQ enhances the accuracy and consistency of diagnosis and ensures that individuals receive appropriate care tailored to their specific needs
| [9] | Karatzias, T., Shevlin, M., Fyvie, C., Hyland, P., Efthymiadou, E., Wilson, D.,... & Cloitre, M. (2016). An initial psychometric assessment of an ICD-11 based measure of C-PTSD: The International Trauma Questionnaire. Journal of Anxiety, Stress, and Coping, 29(5), 561-574. https://doi.org/10.1080/10615806.2015.1100885 |
[9]
.
The Acceptance and Action Questionnaire II (AAQ-II) is the second version of a measure of experiential avoidance and psychological inflexibility. it is constructed of 10 items, and is uses a Likert-type scale that runs from 1 (never true) to 7 (always true), with higher scores indicating greater levels of psychological inflexibility
| [53] | Bond, F. W., Hayes, S. C., Baer, R. A., Carpenter, K. M., Guenole, N., Orcutt, H. K., Waltz, T., & Zettle, R. D. (2011). Acceptance and Action Questionnaire II (AAQ-II) [Database record]. APA PsycTests. https://doi.org/10.1037/t11921-000 |
[53]
.
The Brief Experiential Avoidance Questionnaire (BEAQ) is a 15-item short form of the Multidimensional Experiential Avoidance Questionnaire
| [54] | Schaeuffele, C., Knaevelsrud, C., Renneberg, B., & Boettcher, J. (2022). Psychometric Properties of the German Brief Experiential Avoidance Questionnaire (BEAQ). Assessment, 29(7), 1406-1421. https://doi.org/10.1177/10731911211010955 |
[54]
.
And this study used values bulls – eye the bulls eye living diary using the bulls eye in a diary form may encourage the client to work with values every day, it helps clients get in contact with their valued directions and stimulate activity in those chosen directions
| [55] | Blackledge, J. T., Ciarrochi, J., & Deane, F. P. (2009). Acceptance and Commitment Therapy: Contemporary Theory, Research and Practice: Australian Academic Press. |
[55]
.
2.4.2. Qualitative Tools
Client Change Interview is a semi-structured qualitative instrument, developed by Elliott, Slatick and Urman (2001) with the aim of eliciting the clients’ personal overview and evaluation of their therapeutic experience.
The primary qualitative question guiding this study is: How did the interview contribute to understanding the effectiveness of trauma focused acceptance and commitment therapy to reducing complex ptsd? To answer the main question, an semi structured interview (client change) was used, and open questions which included five questions, The post-interview gave the researchers an opportunity to explore why this program was effective in a depth, And the questions are:
How do you describe your experience of joining the program of trauma-focused acceptance and commitment therapy?
Describe your feelings and thoughts during therapeutic sessions?
In what ways did your involvement in the program contribute to the alleviation of symptoms associated with complex post-traumatic stress? Could you provide specific instances from your personal experience?
How has your life been positively impacted by the Trauma-focused Acceptance and Commitment Therapy program? Please provide detailed explanations.
Would you recommend that others consider enrolling in a trauma-focused acceptance and commitment therapy program? If so, what are the reasons for your endorsement? Additionally, do you perceive any areas within the program that require enhancement and fortification?
2.5. Procedures
Ethical considerations were taken before conduct this study, The study strictly adheres to ethical guidelines and regulations, ensuring informed consent, privacy, and confidentiality of the participants. Collaboration with relevant institutional review boards and ethical committees is in place, including obtaining Helsinki approval.
ITQ, AAQ II, and BEAQ were applied at the beginning and the end of the psychotherapeutic process in after 17 sessions as well as after a 3-month follow-up. And the Comprehensive assessments conducted at various stages of the study: Pre-intervention Assessment: Before initiating therapy, baseline assessments conducted to gauge symptom severity, functional impairment, and overall well-being. Ongoing Assessment: Throughout the therapy process, regular assessments tracked changes in symptoms, functional impairment, and overall well-being. This involved self-report measures associated with ACT principles, clinical interviews, and therapist observations. Post-intervention Assessment: After completing therapy, a final assessment evaluated treatment outcomes.
The participant underwent Trauma-Focused Acceptance and Commitment Therapy (TF-ACT), a specialized approach that blends fundamental ACT principles with trauma-specific techniques. A qualified therapist, experienced in trauma-focused interventions, administer this therapy. The treatment comprised individual sessions conducted regularly, following a personalized treatment plan tailored to the participant's requirements. The therapy's duration depend on clinical progress and individual treatment goals.
And after data analysis and compare the outcomes semi structured and interview conducted.
2.6. Therapeutic Process
The sessions assessment and treatment lasted approximately 5 months by a weekly session, and each session lasted about 60-90 minutes. The therapy sessions created a secure and supportive environment, ensuring confidentiality and a non-judgmental atmosphere. The therapy followed a structured approach, incorporating ACT techniques such as mindfulness practices, defusion, present-moment awareness, self-as-context, values clarification, and committed action. Session notes documented the content of each session, progress made, challenges encountered, and interventions employed.
The session included three stages: living in the present, healing the past, and building the future, The content of the therapy sessions is as follows:
Table 1. Illustrate the sessions.
Summary of the sessions |
First session "Building Rapport" | Obtaining informed consent, Applying ACT scales and Bulls eyes to determine client values. Establishing therapy goals (emotional, behavioral, outcome) by using The “Press Pause”, The Horror Movie metaphors and Magic wand question. Taking history and Detection of traumatic events. |
Second and third session "Psychoeducation" | Training client at Dropping anchor by applying The Emotional Storm Metaphor. Grounding metaphor. Mindfulness breath exercise, and Psychoeducation on trauma (Definition of trauma and trauma-related disorder). Clarifying “complex” trauma and symptoms and Defined Trauma-focused ACT (TF-ACT), Goals, Importance and component of ACT by Showing video about passenger of the bus, The Bear Metaphor, and Monster on a boat metaphors. |
Fourth session Defusion | Training at Dropping anchor through the application five senses mindfulness. Definition of a cognitive fusion and Six categories of fusion: past, future, self, judgments, rules, and reasons. Seeing the true nature of cognitions: that they are nothing more or less than constructions of words and pictures. Clarify the costs of fusion and the aims of defusion and Training defusion from doubt and helplessness, illustrating the costs of experiential avoidance and the benefits of acceptance and applying Helpful Friend and Caveman Mind Metaphors. And practicing these exercises (Hands as Thoughts exercise, Notice, Name, Normalize, Purpose, and Workability strategies and I’m Having the Thought That, Thanking Your Mind. Leaves on a Stream. Thoughts on Paper) in the session and in homework. |
Fifth session Creative Hopelessness and acceptance | Increasing the client awareness of the emotional control agenda and the costs of excessive experiential avoidance, Accepting painful private experiences and Training at the four As of Acceptance and the difference between tolerance and Pseudo-acceptance. Achieving goals through the application of Struggle Switch metaphor, Tug of War with a Monster. Struggling in Quicksand, Kind Hands exercise to foster self-compassion, The wave metaphor, and The weight-lifting metaphor. |
Sixth session "Self-compassion" | Awareness of Self-compassion and difference between self-compassion and self-pity. Defusing from self-judgment (self-criticism, self-loathing, and self-hatred). learning self-motivation through values, values-based goals, and compassionate self-encouragement Dealing with old wounds. And The Two Friends Metaphor (The Two Coaches metaphor). Use Self-Compassion and the Hexaflex. acceptance practice suitable The sky perspective, Kind self-talk. The well-known, Carrot and Stick metaphor, The Orphanage Metaphor |
Seventh session Values, Knowing What Matters" | Discussion about activities the client finds meaningful and Monitoring activity. helps client distinguish between values and outcome goals and setting the SMART goals. Training at values based problem solving The Connect and Reflect exercise. Values cards and checklist. Forty common values sheet. Where You’re Going and How You’re Traveling metaphor. Flavoring and Savoring exercise |
Eighth session Committed action "Doing What Works" | Checking repeatedly that client is willing to take action. Translating values into goals and actions. Overcoming HARD barriers. Facilitating committed action: reframing, reinterpreting, and motivational self-talk. Walking mindfulness. Ten Years from Now, Looking Back The Video of Your Mistakenly Held Funeral One Year from Now “list of pleasant activities” |
Ninth session "breaking destructive patterns" | Discussion any type of problematic, destructive, or self-defeating behavior. Maintaining Change: The Seven Rs reminders, records, rewards, routines, relationships, reflecting, and restructuring the environment. Body scan mindfulness. Functional Analysis Worksheet |
Tenth session "Exposure" | Teaching the client to recognize that she has choices; that there are many ways of responding to these stimuli. Mindfulness in your morning routine. Presence, Control, physical and Willing scales. Exposure Hierarchy worksheet. moving with the TIMES sheet. |
Eleventh session "self as context" | facilitate defusion from self-referential narratives, through conveying the message “you are not your thoughts. Developing the ability to take “the observer perspective,” enabling you to “step back” and observe cognitions without getting caught up in them. and awareness and practicing Mindfulness of a pleasant activities. The Sky and the Weather. The Documentary of You metaphors. The Transcendent Self or “the Observer Self” or “Continuous You” exercise. Good Self/Bad Self exercise. Chessboard and Pieces. The Stage Show of Life |
Twelfth session "sleep, relaxation,,," | Working with the her Body and establish healthy sleep routines, soothe herself when distressed, and relax by Training at relaxation skills and Working with Shame, and applying these metaphors and exercise: Mindful Movement and Stretching, Mindfulness of posture, Mindful self-touch, Kids in the Classroom metaphor and The Swiss Army Knife Metaphor. And handout on “Sleep Hygiene Scrunching Emotions exercise. |
Thirteenth session "relations and Mindful appreciation" | Helping client appreciate her present moment experience, Building Better Relationships and Developing relationship skills and Clarifying Attachment Styles and relationship. and applying Notice five things, active role-play, Attachment Styles handout and Difficult Dilemmas worksheet. |
Fourteenth session “Inner child" | Awareness of grieving and exposure to traumatic memories. practicing forgiving Self and the others by practicing Compassion for the Younger You exercise, move with the TIMES” Test the willingness and CPA. metaphor of “taking a stand” Self-Forgiving and forgive the others. |
Fifteenth session "Ending therapy" | Maintaining Change and Handling Setbacks through drop anchor by applying breath mindfulness, training acknowledge her pain, and respond with kindness; then come back to their values. Preparing Specific Plans (Safety, Relapse Prevention, and Crisis Coping). Exploring posttraumatic growth. And utilizing Safety, Relapse Prevention, and Crisis-Coping Plan sheet, Relapse-Prevention, and the Willingness and Action Plan. Providing of Brief Intervention Toolkit and applying posttest scales. |
Data Analysis: Data analysis conducted employing both quantitative and qualitative methods: Quantitative Data Analysis: Quantitative data from assessments underwent statistical analysis to compare pre-and post-intervention scores and follow up, aiming to assess changes in symptom severity, functional impairment, and overall well-being.
Qualitative Data Analysis: Qualitative data, including therapist session notes and participant feedback, emotion checking record, and patient response analysis in client change interview to identify common change, experiences, and insights related to the therapy process and outcomes.
3. Results
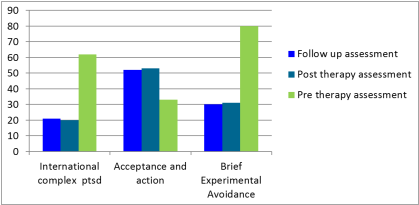
These initial outcomes include comparison of pre- to post-treatment and follow up measurement. And In this single case study that utilized an explanatory sequential design, The first quantitative phase involved the application of the scales (International complex ptsd, Acceptance and action and Brief Experimental Avoidance) and the therapeutic Programme, and the second qualitative phase involved semi structured interview.
3.1. Quantitative Results
The Quantitative data collected from the pre-test, post-test and follow up of Complex PTSD showed significant improvement in the case and reduced symptoms of complex PTSD and in experimental avoidance and a significant improvement in acceptance and action questionnaire, Quantitative analysis was defined as raw scores and percentages.
At pre-measurement, criteria for complex PTSD were applied: P1, P2 > 2 criteria for Re-experiencing here and now met. P3, P4 > 2 criteria for Avoidance met. P5, P6 > 2 criteria for Sense of current threat met. P7, P8, and P9 > 2 meets criteria for PTSD functional. C3, C4 > 2 criteria for Negative self-concept met. C5 and C6 > 2 criteria for Disturbances in relationships met C7, C8, C9 > 2 meets criteria for DSO functional impairment (DSOFI).
Figure 1. Illustrate the most significant difference was observed in the C-PTSD from sever (62 at the pretest 86%) the patient returned to normal in the C-PTSD (20 at the post test, 27%).
And At post-measurement, criteria for complex PTSD were reduced: criteria for Re-experiencing in the here and now (P1, P2) less than 2, Avoidance (P3, P4) less than 2, Sense of current threat (P5, P6) less than 2, PTSD functional (P7, P8, and P9) less than 2 and Negative self-concept (C3, C4), Disturbances in relationships (C5, C6), and DSO functional impairment (C7, C8, C9) less than 1. And This is a strong indication of improvement in the condition as a result of the treatment program. and
figure 1 shows the difference between scales.
3.2. Qualitative Results
we analyzed the client responses using thematic analysis, which is a method for identifying, analyzing and reporting patterns (themes) within data (Braun & Clarke, 2006) and applying Braun and Clarke thematic analysis method is an iterative process consisting of six steps: (1) becoming familiar with the data, (2) generating codes, (3) generating themes, (4) reviewing themes, (5) defining and naming themes, and (6) locating exemplars, The researchers also identified the axes that influenced and achieved change in the case in reducing the symptoms of complex post-traumatic stress disorder, which are (4) axes, which included (11) sub-themes, and are shown in the following illustrative
Table 2.
In the client change interview the patient expected that she will not improve and the change will not happen, because she underwent to previous sessions without any improvement.
although she previous took paroxetine 20 mg once daily without improve, she told no external event responsible for her change, she attribute the change to this intervention.
The patient also expressed her positive view of her, which was changed by therapeutic intervention, as she said, "I was looking at myself negatively and focusing on it more than on my role and my value of life, but with therapy I focus on my worth and my role."
The therapeutic relationship and mutual trust afforded to her by the psychologist had been an assisting aspect of the process of change, providing a comfortable safe place, the role of her husband, who had supported her better before, and the exercise of her homework and various activities, which she considered an essential part of her daily routine.
The patient previously indicated that she might have difficulty adhering to the sessions, but was surprised by the extent of her commitment and her continued presence in each session without being absent.
When she compared herself in the past and now, she not expected this change.
Table 2. Summary of changes reported at post treatment change interview.
Main change | Themes | Case responses |
Daily Routine | Focus on the present moment | She said: “I feel enjoyment in every moment I spend in my life, whether when I wash clothes and dishes, sit with my family, prepare food, or pray.” |
Doing important and valuable work | She said "now I care more about my home and my children than before and try to make them happy" |
Character Development | Learning and Research | She said: "I have taken care of myself and I have been working to develop it, educate myself, adopt books and watch educational and awareness videos close to the field of social service and see videos in the human development". |
Developing capabilities and talents | She mentioned " I felt most confident and felt better about being able to solve problem" |
Reducing Symptoms | Avoidance | She said " sessions made me realistically look at things because at first I was thinking about migration, now I think that this is a reality and I have to live with it and accept it and I don't want to escape and migrate". And she said " when I remember painful memories I applied mindfulness skills" |
Nightmare | " Symptoms of anxiety and stress decreased, nightmares almost faded" |
Threat | She said " Any experience that threatens me, I do not focus on it, but rather I focus on the important value and goals in my life" |
Post-traumatic growth | Gratitude | She said " I appreciate everything in my life even painful memories, because I have a value" |
The Power of Social Relations | "My social relationships have improved and I have visited my relatives and my compliments in their happy events and their joy and sadness. I have become interested in my children and have a lovely time with them and play with them". |
A new perspective on life | she said" At first I was afraid and anxious because I had tried previous therapy sessions and I did not improve, but with the current sessions I realized that there was something changing on my level of thoughts and feelings, thinking positively and accepting difficult events in my life. Negative thoughts and my sad and anxious feelings have decreased". |
Sleep Quality | She said:" Now the anxiety is very weak and I accept it my life and I live my life normally, I sleep normally and I practice mindfulness before sleeping" |
4. Discussion
This study the first study used TF- ACT with C- PTSD as a single case study. We chose this case because she is unique case.
By presenting the results, there are statistically significant differences in reduced symptoms of complex PTSD. and the effectiveness of trauma-focused acceptance and commitment therapy program and can be explained by diverse and structured experiences and meaningful educational attitudes focused on cognitive, emotional and behavioral aspects, Commensurate with the patient's preparedness and abilities as the program included a range of technicians and exercises, training activities, targeted and motivated skills, and positive changes at all levels of knowledge, effectiveness and behavior in the situation; This influenced the acquisition of information and the processing of ideas, organizing emotions and modifying behaviors, trends and achieving desired goals.
The effectiveness of the program is also attributable to the researcher's commitment to applying the principles and ethics of professional work in terms of building the indicative relationship, the indicative contract, the presentation of sessions in a safe environment that allowed the case to express its thoughts, feelings in an environment of trust, reassurance, confidentiality, privacy, mutual respect and comfort, continuous encouragement, exchange of experiences, acquisition and exchange of ideas; This has contributed to motivating the case of sessions and fostering learning.
Furthermore, the case has shown great interest in adhering to sessions with high passion, ensuring early attendance at all sessions without being absent, and committing to carrying out all written, oral, practical and exercise activities both within and outside the sessions, and good cooperation.
The program has achieved great success due to its focus on recovering from the past, living in the present, building the future, and the variety of exercises that focused on enhancing acceptance, reducing experiential avoidance, and living a rich and valuable life.
The role of each component of acceptance and commitment in dealing with complex post-traumatic stress symptoms, Cognitive defusion involves creating space between ourselves and our thoughts and feelings related to symptoms of complex ptsd so that they have less of a hold over us. And defusion skills help to deal with thought, for example helpful friend metaphor, hands as thoughts exercise, I’m having the thought that and thanking your mind, Observing the flow of thoughts (Leaves on a Stream) and Silly voices.
Creative Hopelessness also contributed to increasing the client’s awareness of the emotional control agenda and the costs of excessive experiential avoidance and Accepting painful private experiences through struggle switch metaphor, tug of war with a monster (war)., Struggling in quicksand and kind hands exercise to foster self-compassion and defusing from self-judgment (self-criticism, self-loathing, and self-hatred) and dealing with old wounds.
Clarifying the values and committed action helped the patient overcome the traumatic events and focus on the different values, such as caring for her children, loving learning, and taking care of her health. In addition to the patient's exposure training made her focus on behaviors that validated her value while she remembered the war and the sounds of frightening flying.
Mindfulness exercises played a crucial role in her living in the moment and not passing judgment on her experience, which increased her efficiency in living a rich life such as Mindfulness in your morning routine, pleasant activities, movement and stretching, body scans, mindfulness of posture and mindful self-touch.
Self as context metaphors and skills facilitate defusion from self-referential narratives, through conveying the message “you are not your thoughts '' and developing the ability to take “the observer perspective,” enabling you to “step back” and observe cognitions without getting caught up in them. And these exercises are the sky and the weather, the transcendent self or “the observer self” or “continuous you” exercise. And this program focuses on improving sleep quality, and training relaxation through establishing healthy sleep routines, self-soothing when distressed. And helping clients appreciate their present moment experience and building better relationships and developing relationship skills.
Inner child helps to understanding how past trauma affects to present behavior, developing healthy coping mechanisms, improved emotional regulation and increased self-esteem, self-compassion, and compassion for others such as compassion for the younger you exercise. Finally this program promotes positive feelings towards self and others through Forgiving and empowering the patient in the face of future events by preventing relapse and Crisis Coping.
Integration of Qualitative & Quantitative Findings:
By presenting quantitative and qualitative results, qualitative results supported quantitative results, and explained the depth of improvement in the patient. The change that emerged from the change interview are consistent with the high degrees of improvement in the patient, and the patient's responses emphasized the reduction of avoidance and night nightmares as well as the improvement of her social relations and functional performance, and substantial changes in the patient's life.
The results of the current study supported the results of these studies which have proven the effectiveness of ACT in dealing with symptoms of trauma such as Colleen & Kirsch Hiltz White
| [45] | Kirsch Hiltz White, C. M. (2020). Comparison study: Trauma-focused cognitive behavioral therapy and acceptance and commitment therapy for trauma. |
[45]
, Ramirez et al.
| [46] | Ramirez, M. W., Woodworth, C. A., Evans, W. R., Grace, G. A., Schobitz, R. P., Villarreal, S. A., Howells, C. J., Gissendanner, R. D., Katko, N. J., Jones, K. N., McCabe, A. E., & Terrell, D. J. (2021). A trauma-focused intensive outpatient program integrating elements of exposure therapy with acceptance and commitment therapy: Program development and initial outcomes. *Journal of Contextual Behavioral Science, 21*, 66-72. https://doi.org/10.1016/j.jcbs.2021.06.002 |
[46]
, Spidel et al.
| [44] | Spidel, A., Daigneault, I., Kealy, D., & Lecomte, T. (2019). Acceptance and commitment therapy for psychosis and trauma: Investigating links between trauma severity, attachment, and outcome. *Behavioural and Cognitive Psychotherapy, 47*(2), 230-243. https://doi.org/10.1017/S1352465818000413 |
[44]
. Qualitative results also showed a topic related to post-traumatic growth and this is consistent with a study Troxel-Galang
| [47] | Troxel-Galang, A. (2021). *The efficacy of a spiritual acceptance and commitment therapy protocol for post-traumatic growth* (Unpublished doctoral dissertation). The Wright Institute. |
[47]
, that has demonstrated the effectiveness of ACT in improving post-traumatic growth. Also supported the results of Orsillo and Batten
| [36] | Orsillo, S. M., & Batten, S. V. (2005). Acceptance and commitment therapy in the treatment of posttraumatic stress disorder. *Behavior Modification, 29*(1), 95-129. https://doi.org/10.1177/0145445504270876 |
[36]
study of the results of the current study.